Two federal departments have spent over $50 million since 2015 on
hotel bookings for migrants illegally crossing the Canadian border and
also for lawful refugee applicants, new government figures show.
In an Inquiry of Ministry recently tabled in the House of Commons,
the Department of Immigration and Department of Public Works said they
have paid a combined $50.6 million since November 2015 on the hotel room
bookings, according to Blacklock’s Reporter.
The inquiry showed that over 63,700 foreigners stayed in the hotel rooms, with over 26,300 of them being illegal immigrants.
“How many hotels has the government contracted for housing asylum
seekers or refugees?” she asked in the inquiry, while also requesting a
breakdown of the hotel bookings “by city or municipality” and for the
contracts pertaining to each.
The two departments said they signed contracts with a total of 35 hotel operators in cities across Canada, but most were located in Ontario and Quebec.
The Dev Hotel and Conference Centre in Cornwall, Ont., received the
largest contract at $30 million, with the next biggest going to
the Quality Hotel & Suites Toronto Airport East for nearly $3
million.
Travelodge Montréal Airport received a contract worth just under $2
million and the Marigold Hotel in Brampton, Ont., received a $1.2
million contract.
Rempel Garner also wanted to know how many of the migrants staying in
the hotels had claimed asylum after entering Canada “irregularly”
through the unofficial border crossing at Roxham Road in Quebec, but the
inquiry did not specify.
Irregular Migration
The total cost to government of illegal immigration into Canada has still not been estimated by any federal office or agency.
However, the Parliamentary Budget Office (PBO) estimated in 2018 that
the figures were likely around $1 billion over every three
years—equalling a total average of over $14,300 for every illegal
immigrant.
“There has been a recent increase in the number of asylum claimants entering
Canada via its southern border,” said the 2018 report, titled “Costing Irregular Migration across Canada’s Southern Border.”
“For an irregular migrant that entered Canada in 2017-18, the PBO
estimates that the cost to the federal government can vary between
$9,915 and $33,738.”
The PBO added in the report that it “undertook a sensitivity analysis
of future variable costs relating to irregular migration” to project
how costs could change in the near future.
Assuming the number of irregular migrants to be higher or lower by
10,000 relative to the number in fiscal year 2017-2018, the PBO
projected that the costs would rise steadily year over year and reach
over $600 million for the fiscal year 2019-2020.
Do you know when Paxlovid should be used to treat COVID-19?
Are you aware of the reasons for the mixed results of its phase 2 and
phase 3 clinical trial data versus its real-life studies? Do you know
what the most significant concern about Paxlovid is for its future
application in treating COVID-19?
Reputed as a so-called “game-changer” oral antiviral pill to treat
COVID-19, Paxlovid can prevent hospitalization and death in people who
are at high risk of severe COVID-19. However, you should know that the
research findings on Paxlovid are not always what they seem to be.
We will provide a balanced, unbiased review related to Paxlovid’s
development history, clinical trial and real-world effectiveness data,
and the drug’s advantages and limitations. We will also clarify the
connection between oral antivirals and human immunity.
Summary of Key Facts
Paxlovid Is Not Yet Approved by the FDA
Paxlovid Should Be Used Soon After Virus Infection
Clinical Trial: 89 Percent Efficacy With Side Effects of Dysgeusia and Diarrhea
Paxlovid Doesn’t Work in Younger Patients
In a Real-World Study, Paxlovid Has Shown Limited Effectiveness
Finding “Treatable” Patients Has Proven Challenging
Drug Resistance Is a Major Concern
Another Major Concern Is Paxlovid’s Interaction With Other Drugs
Natural Immunity Influences the Success of Paxlovid and Other Antivirals
Pfizer’s Paxlovid contains two active ingredients. The first is
nirmatrelvir (PF-07321332), a protease inhibitor that interrupts the
viral replication cycle.
The action of viral protease
is like a pair of scissors in the hands of a tailor. The protease can
cut the long synthesized viral protein (like a piece of cloth) into
various fragments with different functions. The virus will combine these
protein fragments into a complete virus particle.
On June 30, 2022, Pfizer filed a New Drug Application (NDA) with the
FDA, seeking approval for Paxlovid. As of today, however, it has not
been approved by the FDA for the treatment of COVID-19.
2. Paxlovid Should Be Used Soon After Virus Infection
A group of researchers, mainly from Pfizer Worldwide Research, published an article in Science
on Nov. 2, 2021, about the discovery and characterization of Paxlovid.
In vitro antiviral activity of Paxlovid has been evaluated in multiple
cellular models. In vitro testing showed that Paxlovid demonstrated
potent antiviral activity against SARS-CoV-2, MERS-CoV, and other
similar coronaviruses.
However, the researchers noted that Paxlovid should be given very soon after a subject is infected with COVID-19.
When given to mice as early as four hours after infection with
SARS-CoV-2, a 300 or 1,000 mg/kg treatment of Paxlovid was effective in
reducing the SARS-CoV-2 viral load in the lungs.
This means Paxlovid should be taken as early as possible post-virus
infection. That is also the rationale for the inclusion criteria: only
patients within five days of symptom onset were recruited in phase 2 and
phase 3 clinical trials. In other words, if the viral infection is in a
late stage and the illness is more severe, Paxlovid may not be as
helpful as it is for early infection.
3. Clinical Trial: 89 Percent Efficacy With Side Effects of Dysgeusia and Diarrhea
The findings
of phase 2–3 double-blind, randomized, controlled trial supported by
Pfizer were published on Feb. 16, 2022, in the New England Journal of
Medicine.
The trial involved 2,246 symptomatic, unvaccinated, non-hospitalized
adult patients who were at high risk for developing severe COVID-19
symptoms, and symptom onset was no more than five days. They were
randomly selected to receive either Paxlovid 300 mg with other standard
care or a placebo with other traditional medicine twice a day for five
days.
The final analysis, involving 1,379 patients, showed that Paxlovid
reduced the risk of COVID-19-related hospitalization or death by 89
percent, compared to the placebo group when given less than five days
after symptom onset.
The main side effects observed with Paxlovid vs. control were
dysgeusia (a taste disorder, 5.6 percent versus 0.3 percent) and
diarrhea (3.1 percent versus 1.6 percent), both higher than the placebo
group. This indicates potential side effects on the neurological and
gastroenterological systems.
Again, consistent with the development concept of this drug and
aligned with its animal data, the drug has to be taken at an early stage
of infection. Most patients (66.3 percent) received the first dose of
the trial drug or placebo within three days after the onset of symptoms.
In the real world, not many patients can take the drug in the first
onset days, especially during the current Omicron era, as most patients
may view their symptoms as a common cold and may not be aware of having
contracted COVID-19.
4. Paxlovid Doesn’t Work in Younger Patients
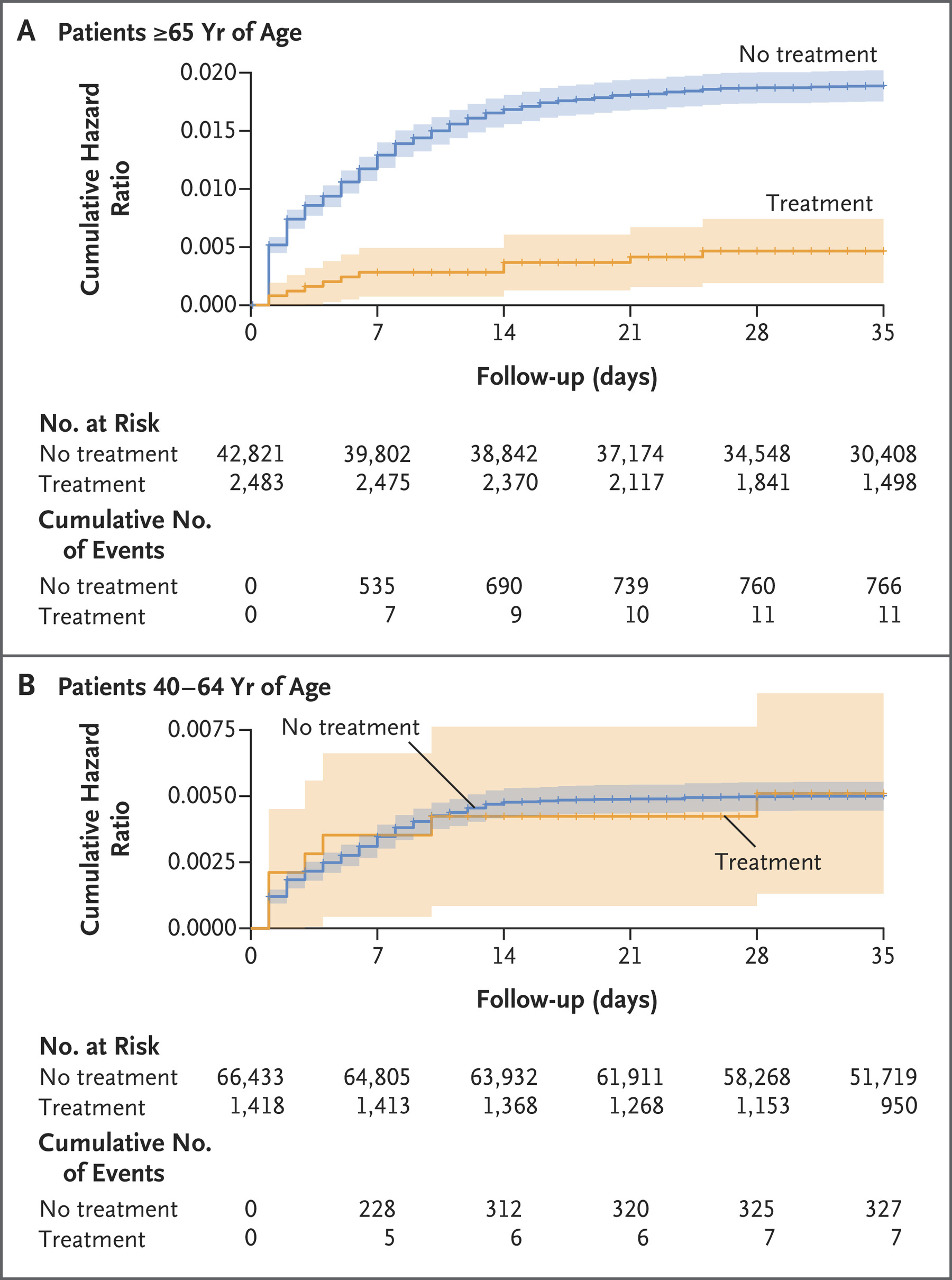
A large-scale observational, retrospective cohort study involving more than 100,000 subjects conducted in Israel during the Omicron-surge phase was published in the New England Journal of Medicine on Sept. 1, 2022.
This study was based on data obtained from a large health care
organization covering approximately 52 percent of the Israeli
population.
The research took place while the Omicron variant was dominant; the study period started on Jan. 9, 2022, and ended on March 31, 2022.
Cumulative Hazard Ratio for hospitalization due to Covid-19, according
to age group and treatment status. (New England Journal of Medicine)
Researchers found that among patients 65 years of age or older,
Paxlovid can lower the risk of hospitalization by 73 percent, and reduce
the risk of death by 79 percent. There was, however, no evidence of a
benefit found in 40- to 64-year-old adults.
5. Finding “Treatable” Patients Has Proven Challenging
We may wonder why Paxlovid works in elderly patients but not in the younger group of people in the Israel study.
Paxlovid has a narrow treatment window (five days after symptom
onset) and a relatively short treatment period (five days only). Phase 2
and 3 trials are conducted in a selected group of patients in a
controlled study setting. However, real-life studies may not be able to
replicate the same criteria as phase 2 and phase 3 trials do—all this
results in limitations for the clinical application of Paxlovid and mixed efficacy data.
First, the drug has to be taken by a patient as early as possible
after SARS-CoV-2 infection. This is based on a list of factors involving
the drug’s mechanism of action, development concept, preclinical study
dosing timing, and the phase 3 study design. It’s also common sense that
earlier treatment offers a better outcome.
However, it has been reported by a Johns Hopkins study that the “gold standard” COVID-19 PCR test has false negative rates ranging from 20 to 66 percent. The false negative rate of the SARS-CoV-2 PCR test is much higher during earlier infection days than later. It
can be up to 100 percent on the first day and down to 20 percent on the
eighth day of exposure (typically the third day of symptoms).
A systematic review
of 34 studies enrolling 12,057 COVID-19-confirmed cases revealed
that up to 54 percent of COVID-19 patients might have an initial
false-negative RT-PCR result.
This results in a dilemma: on the one hand, we have to start
treatment. On the other, the high false-negative rate hampers early
Paxlovid application in the maximal patient population.
Paxlovid is not indicated for treating COVID-19 patients who require
hospitalization due to severe or critical COVID-19 diseases. Based on
previous clinical trial data, none of those trials were conducted in
severe COVID-19 patients, so it is essential to bear this point in mind.
Furthermore, Paxlovid is not indicated for mild-to-moderate COVID-19 patients. Patients must present a high risk of progressing to severe diseases,
including but not limited to older age, underlying medical conditions
of cancer, diabetes, chronic lung diseases, or chronic kidney diseases.
Additional data support its use past five consecutive days. These
factors together indicate that finding suitable test subjects has proven
difficult.
6. In a Real-World Study, Paxlovid Has Shown Limited Effectiveness
In October 2022, Hong Kong University researchers compared the
clinical effectiveness of two oral antiviral drugs, Paxlovid and
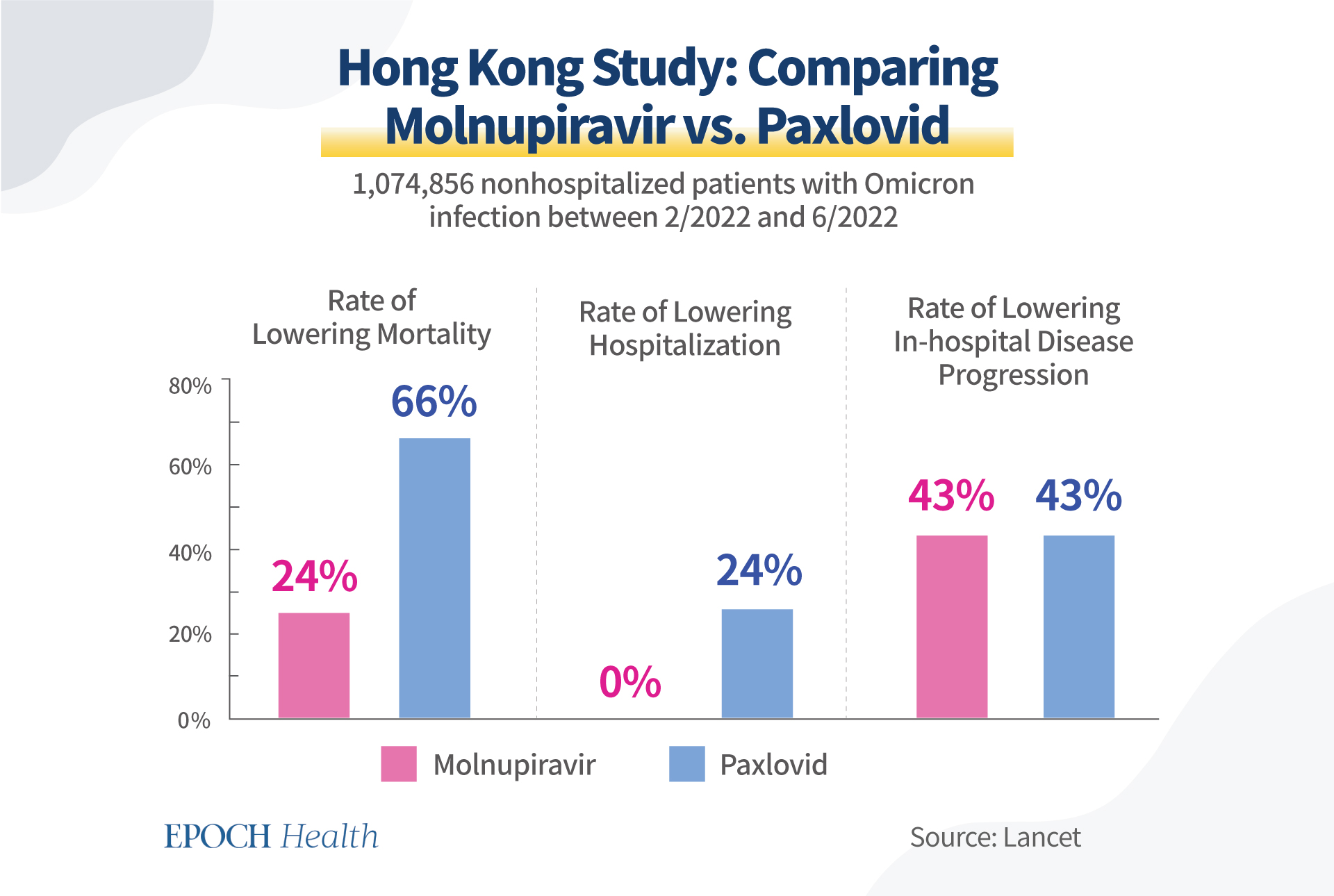
molnupiravir, among Hong Kong residents. The researchers’ observational study was published in The Lancet.
Between Feb. 26 and Jun. 26, 2022, among the 1,074,856
non-hospitalized patients infected with Omicron, 6,464 were treated with
Paxlovid and 5,383 with molnupiravir. Compared to the Paxlovid group,
the molnupiravir group consisted of older and more unvaccinated
patients.
It is worth noting that these two antivirals were not compared
directly in this study, but each was compared to its control group with
matching patient conditions.
Paxlovid reduced the mortality rate by 66 percent versus the control,
while molnupiravir lowered the mortality rate by 24 percent versus its
own control.
Molnupiravir did not lower hospitalization rate, while Paxlovid lowered the hospitalization rate by 24 percent.
Molnupiravir lowered in-hospital disease progression by 43 percent, while Paxlovid also decreased it by 43 percent.
None of these rates look as good as Paxlovid’s phase 2 and phase 3
clinical trial data. One of the most likely reasons is how well the
narrow treatment window of the drug has been followed, i.e., only five
days after symptom onset.
Hong Kong study results on the effectiveness of Paxlovid and molnupiravir. (The Epoch Times)
7. Drug Resistance Is a Major Concern
Antiviral treatments are often associated with the development of
drug-resistant viruses. There is a well-known saying in the antiviral
community: “No antiviral, no resistance.”
A virus is a cunning microorganism. When you add pressure to its
replication cycle, a virus will typically find a way to detour by
mutating and will manage to survive. This is the primary mechanism of
antiviral resistance.
There are already quite a few lab research studies indicating
SARS-CoV-2 could mutate to bypass the drug target, i.e., reducing the
efficacy of the drug in actual clinical usage, as reported by Science in June 2022.
In this sense, Paxlovid is no different than other antivirals.
Even though researchers reported that nirmatrelvir remained effective in multiple variants of SARS-CoV-2,
including Alpha, Beta, Delta, Gamma, Lambda, and Omicron, as well as
the original strain, this does not mean that the drug will be effective
against future variants of the virus.
Two research groups have independently shown that SARS-coV-2 quickly gains the ability to avoid nirmatrelvir’s attack.
One study was led by virologist Dirk Jochmans from Belgium,
who found that after a dozen rounds of nirmatrelvir treatment,
SARS-CoV-2 developed three mutations—at positions 50, 166, and 167 of
the critical protease Mpro—that reduced the virus’ susceptibility to
nirmatrelvir 20-fold.
Judith Margarete Gottwein led the other studyat
the University of Copenhagen. She spotted resistance-conferring
mutations at similar positions 50 and 166 in Mpro, conferring 80-fold
reduced susceptibility to nirmatrelvir.
What’s more shocking is the fact that two of the mutations (166 and 167) flagged by the Belgian group were already reported to be circulating in people according to a preprint of research findings by United States scientists posted on May 30, 2022.
As a result of this concern, patients under the use of Paxlovid
should be regularly monitored for antiviral resistance, especially when
signs of rebound or reinfection appear.
8. Another Major Concern Is Paxlovid’s Interaction With Other Drugs
CYP3A breaks down Paxlovid. CYP3A is one of the most important enzymes in our liver and digestive tract, which play a significant role in breaking down the drug.
Potent CYP3A inducers will reduce the drug exposure of Paxlovid,
resulting in loss of response to Paxlovid treatment and increased risks
of drug resistance.
Paxlovid is contraindicated with a long list of drugs of CYP3A inducers, partially due to the concern of potentialantiviral resistance.
9. Natural Immunity Influences the Success of Paxlovid and Other Antivirals
Even though we applaud the
efforts by the pharma industry to develop antivirals, we should not
forget those limitations. Furthermore, a well-functioning immune system
is necessary for an antiviral drug to exert its effect.
The main merit of antiviral drugs is that when the body’s immune
system is not strong enough, external drugs can temporarily inhibit the
replication of the virus, giving our natural defense system some time to
recover to its full strength.
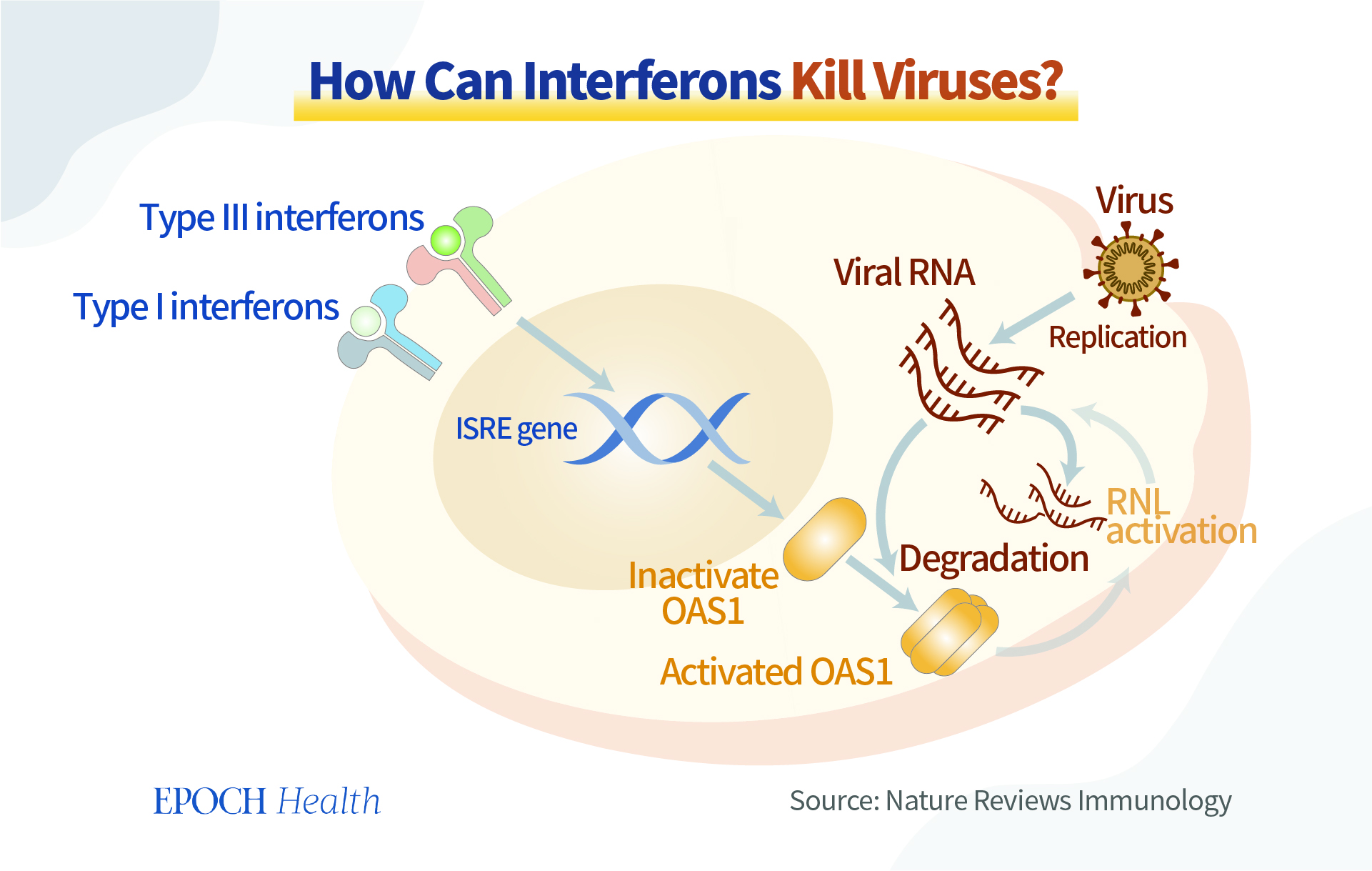
Meanwhile, we should not neglect the ability of our bodies to produce
antiviral substances. Interferon, for example, is produced by many
immune cells (white blood cells, NK, NKT, and T cells). As the name
implies, through “interference,” it achieves antiviral effects.
Interferon is like a commander, giving instructions to coordinate
various cells and signaling pathways to work together to fight a virus.
There are many ways to strengthen the amount and maximize the potential of the natural antiviral substances that our bodies make.
Interferons interfere with the replication of the virus. (The Epoch Times)
Natural immunity is an endogenous antiviral force in our body, like a
joint force ready to fight against invading pathogens. If we are
mindful enough to nourish our immunity in peaceful times, the defense
mechanisms will work well when the “war” comes.
In summary, we should calmly view the strengths and limitations of
antiviral drugs. On the one hand, we expect antiviral drugs to work
well; on the other hand, we must enhance our immune system’s power to
resist the virus in a more natural, systematic, dynamic, and resourceful
manner.
It sounds counterintuitive. However, there are many reasons why there
is a lack of study, including this cancer’s aggressive nature, poor
survival rate, and the great differences in how it presents across
countries and even between sexes.
Esophageal cancer is not as common in the United States. However, a 2022 analysis presented at a conference
found that from 2012 to 2019, the rate of esophageal cancer for people
ages 45 to 64 almost doubled, based on 5 million people’s data in
Florida.
Esophageal Cancer Is One of the Least Studied Common Cancers, 3 Reasons
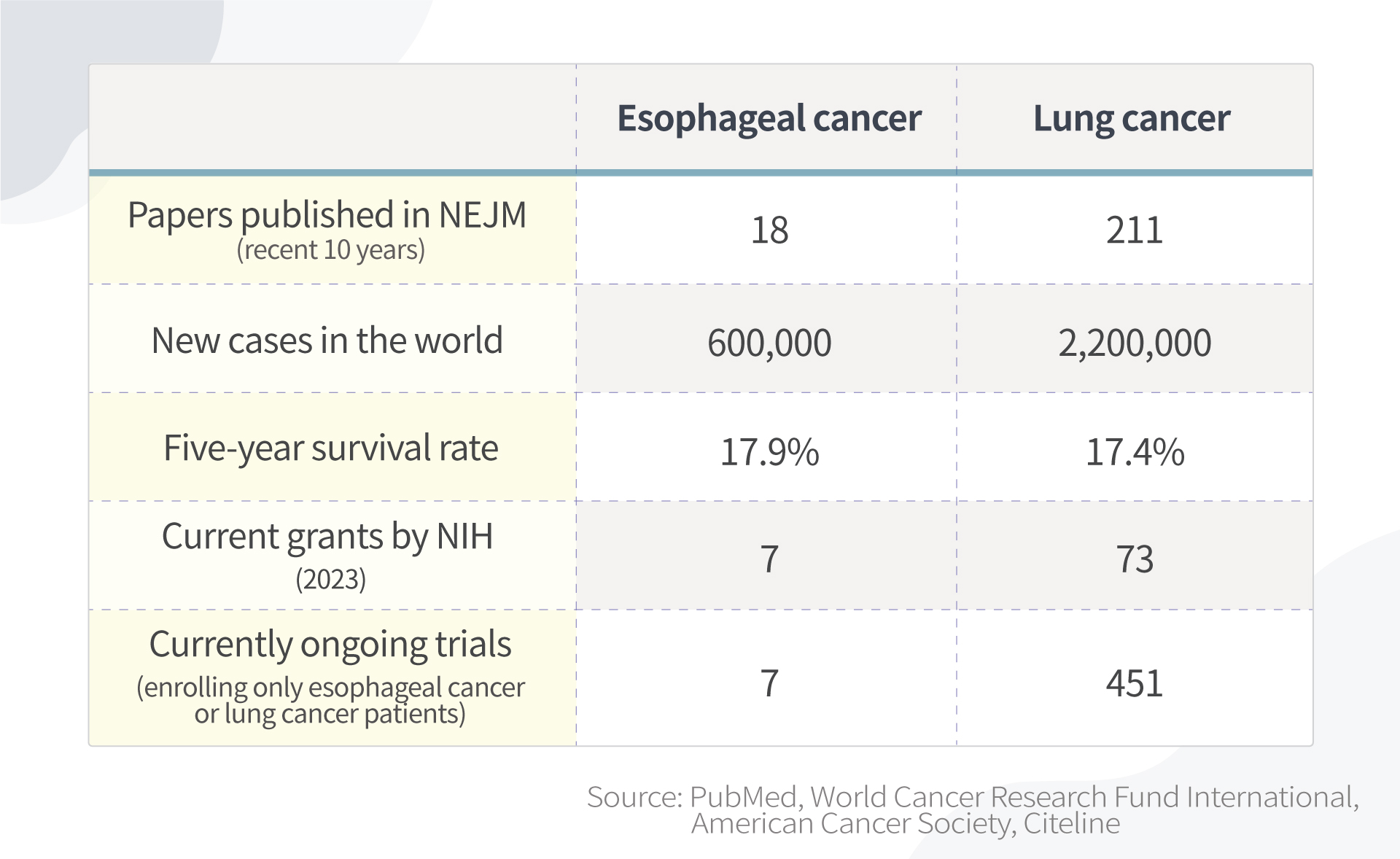
By searching publications in the New
England Journal of Medicine, the world’s leading medical journal,
studies in esophageal cancer are far fewer than those in lung cancer.
Studies in esophageal cancer are far fewer than those in lung cancer. Information accessed February 2023. (The Epoch Times)
There are multiple reasons for this:
1. Incidence rates are relatively low in the United States
The majority of esophageal cancer cases are outside of the United States. Esophageal cancer makes up only about 1 percent of cancer cases in the United States.
The National Institutes of Health (NIH) is the world’s largest public
funder of biomedical research. However, because esophageal cancer is so
uncommon in the United States, it is difficult to be granted funding
from institutions like NIH to research it.
Also, because there aren’t many esophageal cancer patients in the
United States, there is less motivation for pharmaceutical companies to
develop new drugs targeting esophageal cancer.
2. Presents differently between sexes and among races, but root causes unknown
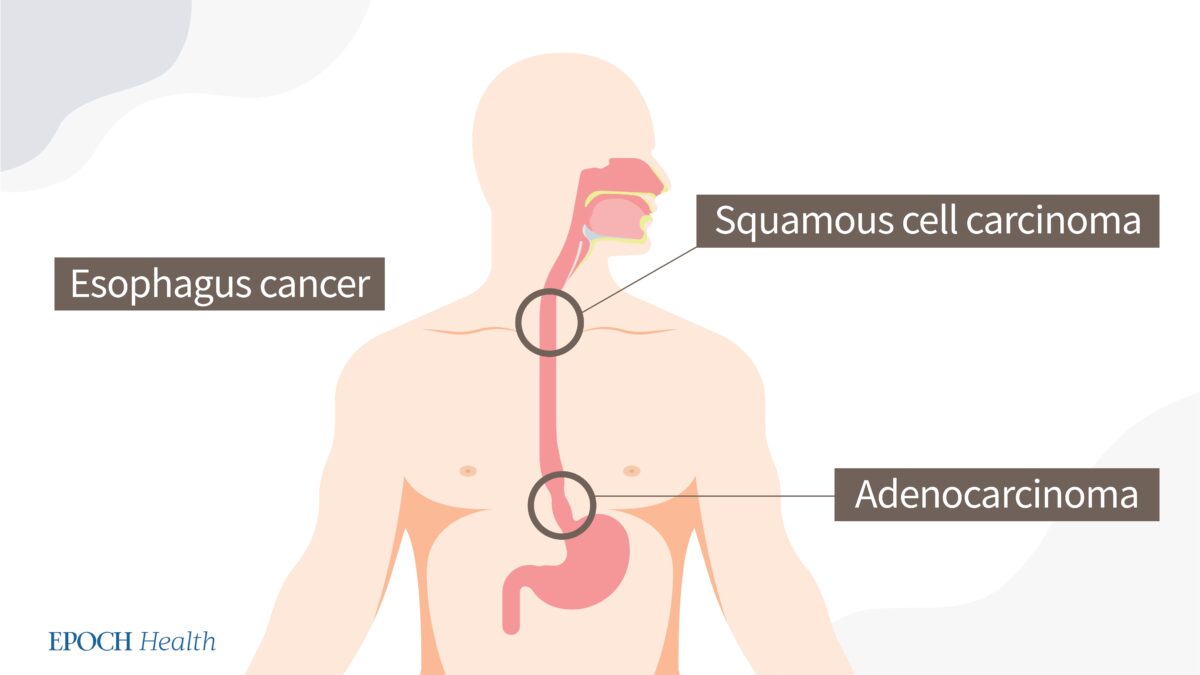
Most esophageal cancers can be classified as one of two types: adenocarcinoma or squamous cell carcinoma.
Squamous cell carcinoma is the predominant histological type
worldwide. This form mainly occurs in the “Asian Esophageal Cancer
Belt,” which includes China.
However, in countries like the United States, Australia, the UK, and Western Europe, adenocarcinoma incidence is higher.
Two types of esophageal cancers. (The Epoch Times)
Similar to other cancer types, esophageal cancer exhibits sex
disparities in occurrence. The incidence of esophageal adenocarcinoma is
about eight times higher (pdf)
in men than in women. Sex is known to be an independent prognostic
marker for squamous cell carcinoma but not for adenocarcinoma, with
survival rates being higher in women.
Esophageal cancer affects races differently, as well. While nonwhite patients
were more likely to develop squamous cell cancer or a tumor in the
middle esophagus, white patients were more likely to develop
adenocarcinoma or a tumor in the lower esophagus. The root causes for
these differences are still unknown.
Esophageal cancer is very complicated and differs across sex, race,
region, and socioeconomic status. Thus, as the number of patients in the
United States is limited, and with so many factors to consider, it is
hard to get statistically significant results.
3. High death rate
On average, according to a paper published in the World Journal of Gastroenterology, about 40 to 45 percent of patients
die within a year after diagnosis, so it is hard to recruit patients
for studies if they are too sick. This contributes to a limited number
of eligible patients.
Can Esophageal Cancer Be Identified Early?
The deadliness of cancer depends on when it is found. If esophageal
cancer is found while it is still localized, the patient has a 46 percent chance of survival for
five more years. If it is found while it is regional, that chance drops
to 26 percent, and if found while distant, only 5 percent of patients
will survive five more years.
Localized means that the cancer is growing only in the esophagus.
Regional means that the cancer has spread to nearby lymph nodes or tissues.
Distant means that the cancer has spread to organs or lymph nodes away from the main tumor.
Unfortunately, in the earliest stages when it’s easiest to treat,
esophageal cancer has very few symptoms. Therefore, it is called a
silent killer.
Can screening be done? In the United States, screening for esophageal
cancer is not recommended, partially because the incidence is low;
therefore, for society overall, it is not cost-effective at lowering
risk.
Will There Be a Sharp Increase in Esophageal Cancer in the US?
The researchers who presented their findings at the 2022 Digestive
Disease Week conference argue that more middle-aged persons should be
checked for esophageal cancer in light of their study, as esophageal
cancer may be increasing among middle-aged people.
That being said, the study’s findings should be analyzed with
caution, as the study only included adults residing in Florida, meaning
it’s not wholly representative of the population of the United States.
For instance, the increase might be due to Florida’s growing population
(it has grown by 14.6 percent
in the last decade and growth accelerated during the pandemic).
Florida’s late-night eating habits may also influence the increase;
Miami is a late-night eating town compared to the rest of the country.
More on this later.
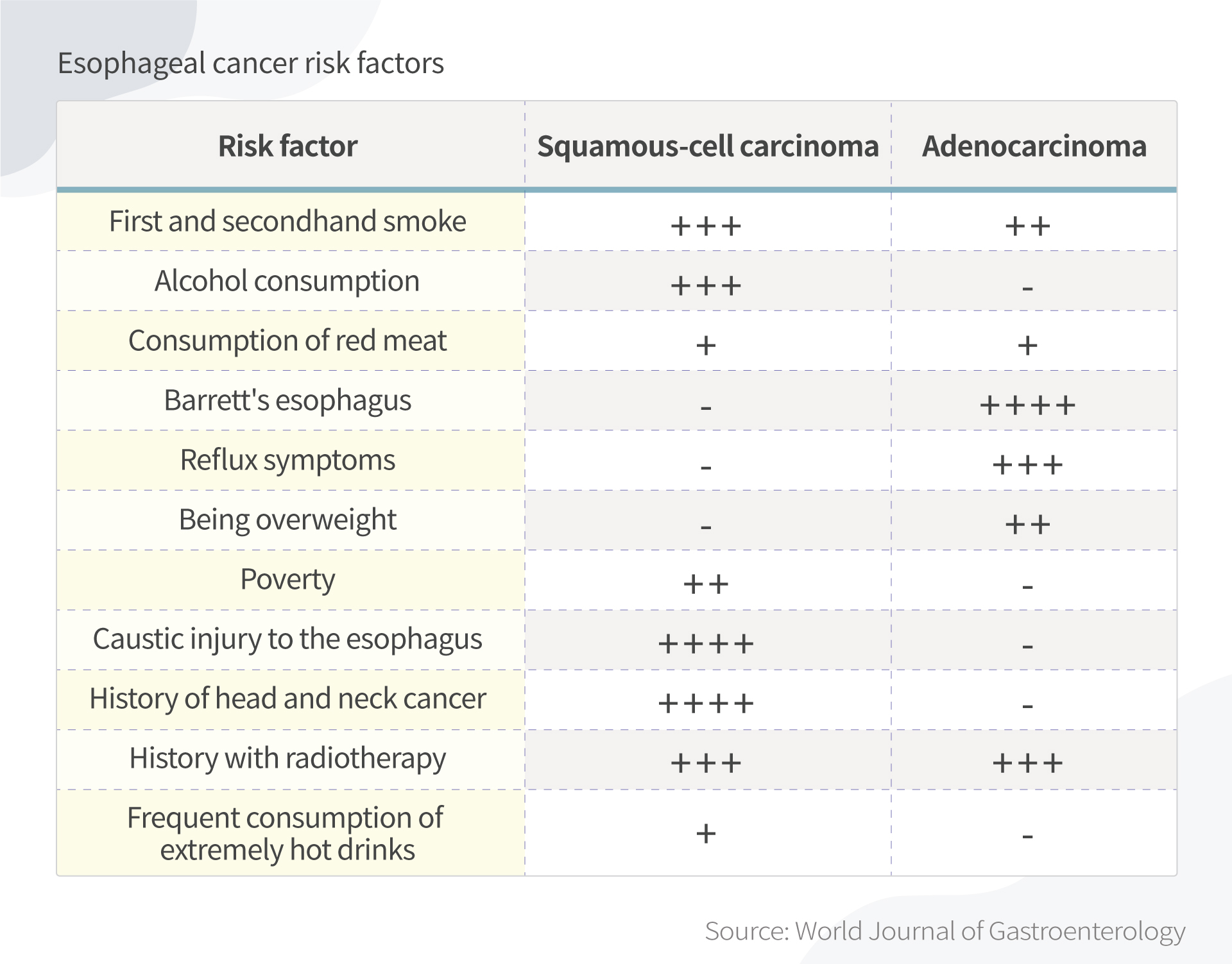
What Are Common Risk Factors of Esophageal Cancer?
As mentioned, nearly half of the patients die within a year once they are diagnosed—which is why prevention is very important.
Smoking, alcohol, obesity, drinking hot tea, red meat consumption,
poor oral health, low intake of fresh fruit and vegetables, and low
socioeconomic status have all been associated with a higher risk of
esophageal cancer, according to the World Journal of Gastroenterology
paper.
Risk factors of adenocarcinoma and squamous cell carcinoma. (The Epoch Times)
5 Ways to Prevent Esophageal Cancer
There are a few things that you can do now to lower your chance of developing esophageal cancer.
1. Avoid eating late
When you eat late at night and then lie down, the contents of your
stomach press harder against the lower esophageal sphincter. This can
trigger gastroesophageal reflux disease (GERD), or acid reflux. Some ways to avoid this include:
Waiting two to three hours after eating to go to bed.
Not snacking late at night.
Eating larger meals earlier in the day. Try to make your last meal small.
Many people love to have late-night dinners and drinks, especially
while on vacation. Although having to restrain yourself from delicious
food at night might be hard, it is rewarding to control your weight and
prevent other diseases beyond esophageal cancer.
2. Avoid hot foods and liquids
Different people have different eating habits. I hear discussions
about why Chinese people like drinking hot water. It can be relaxing and
soothing. However, drinking very hot beverages may be associated with esophageal cancer risk.
Thermal irritation has long been known to be a risk factor. Back in
the 1930s, after reviewing clinical records of 771 cases of esophageal
cancer, New York physician W.L. Watson wrote that
“thermal irritation is probably the most constant factor predisposing
to the cancer of the esophagus.” This prevalence could explain why a
large proportion of all cases of esophageal cancer affects populations
in which drinking tea, coffee, or maté, or eating hot foods is common.
Decades later, this conclusion is supported by multiple studies. More recently, the World Health Organization, a 2018 Chinese study, and a 2019 Iranian study all hinted at the connection.
It should be noted that some studies used a temperature greater than
which most people would normally drink liquids. Still, drink liquids at a
reasonable temperature.
3. Avoid smoke and alcohol
Drinking alcohol and smoking are major risk factors for esophageal cancer, especially in Western populations, as established by many retrospective studies.
The observed association between smoking and adenocarcinoma risk is
weaker than that for squamous cell carcinoma, while the effect of
alcohol on adenocarcinoma is uncertain.
Notably, any level of alcohol consumption
increases esophageal cancer risk. The more a person drinks, the higher
their risk. Compared to no alcohol consumption, heavy drinking leads to a
five-fold increased risk.
4. Beware of Barrett’s esophagus
One of my studies on esophageal cancer started with a patient with a
family history of esophageal cancer. He originally had Barrett’s
esophagus and later developed esophageal cancer.
Barrett’s esophagus—which usually results from acid reflux—is
recognized as a risk factor for esophageal cancer. Acid reflux damages
the esophagus, resulting in the lining thickening and turning red.
Between 5 and 8 percent of persons with acid reflux develop cancer.
The sole indicator still effective for determining whether people are
at an elevated risk of developing cancer is the presence of
precancerous cells (dysplasia) in Barrett’s esophagus.
But don’t worry. The diagnosis of Barrett’s esophagus should not be a
reason for alarm. If it coincides with high-grade dysplasia, your
doctor might recommend a minimally invasive esophagectomy.
Furthermore, recent research (pdf) has shown that under the right conditions, Barrett’s esophagus can be made to regress after endoscopic ablative therapy.
5. Boost your immune system
Before I started my research in gastrointestinal cancer, I worked at a
Chinese medicine hospital and heard a story from my supervisor about
his friend, who happened to be my previous neighbor. He had developed
esophageal cancer at a young age and was hopeless. He then took ginseng
and had a fever for days. He lost consciousness and after he woke up, he
was cancer free.
I am not encouraging readers to take ginseng to prevent esophageal
cancer without consulting Chinese medicine doctors. Plus, different
ginseng has different effects.
Takeaway
According to the study using electronic health records in Florida,
esophageal cancer is on the rise among middle-aged Americans. Since this
is a deadly cancer that is hard to diagnose early, be aware of any
early signs, such as difficulty swallowing (dysphagia), weight loss
without known reasons, chest pain, pressure or burning in your
esophagus, and talk to your doctors as early as you can.
The most important thing you can do today is to have a healthy
lifestyle and a positive outlook, get rid of bad habits, and manage
stress to ensure you have a good immune system.